The Regional Hospital of Bellinzona and Valleys has integrated in-situ simulation into clinical risk management, transforming it from a training tool into a strategic lever for process improvement. With the SIMPASS project, developed in collaboration with the Cantonal Simulation Center, the ORBV has adopted a proactive approach to safety based on structured debriefings, analysis of contributing factors, and resilience building. This concrete experience demonstrates how simulation can become a driver of systemic learning and a pillar of safety culture in healthcare.
From human error to system resilience
According to renowned psychologist James Reason, human error is universal and inevitable; it can be reduced but never eliminated. However, errors also offer valuable learning opportunities to prevent them from recurring at the individual, team, and system levels. Healthcare organizations must create optimal working conditions and implement measures to reduce the likelihood of errors. Traditionally, risk management has focused on standardization to reduce human variability, assuming that strict adherence to procedures ensures safety. However, the Safety-II (Hollnagel) approach recognizes that adaptability is critical to system resilience. On-site simulation provides healthcare professionals with a safe environment to hone their technical and non-technical skills, promoting communication, leadership, and teamwork directly in their clinical environment, improving patient safety and quality of care. Patient safety therefore benefits greatly from simulation programs, and simulation is now considered an integral part of clinical risk management. A healthcare system demonstrates a high level of maturity in risk management when simulation is used not only to train individual operators, but also to test systems, identify vulnerabilities in processes, and prevent adverse events before they occur in real patients.
Simulation and clinical risk: integration at the Bellinzona and Valli Regional Hospital
At the Bellinzona and Valli Regional Hospital (ORBV), it all began in 2021, when, with the collaboration of the Cantonal Simulation Center (CeSi), in-situ simulation practices began to be combined with the risk management activities of the Quality and Patient Safety Service. This cultural and methodological transformation has led to the gradual integration of in situ simulation with clinical and organizational risk management methodologies. The aim of this approach is to anticipate critical issues and strengthen psychological safety within teams.
The ORBV is a strategic facility within the Cantonal Hospital Organization (EOC), the multi-site public hospital network of the Canton of Ticino, Switzerland, which has a total of approximately 1,000 beds. The ORBV provides a wide range of services, including emergency care, general hospital care, and specialist services at the regional and cantonal levels. The facility houses nationally renowned centers of excellence, such as the Oncology Institute of Southern Switzerland (IOSI) and the Pediatric Institute of Southern Switzerland (IPSI). In 2024, the hospital handled 12,639 admissions, 265,902 outpatient consultations, and performed 8,089 surgical procedures. With a staff of 1,830, including 430 doctors and 816 nurses, the ORBV remains a cornerstone of high-quality care and support for the local population.

The ORBV’s journey has not been straightforward but rich, born in the field, from experimenting with various approaches and listening to the real needs of the teams, and which today takes the form of an integrated approach to simulation at the service of risk management activities to improve clinical and organizational processes.
The birth of SIMPASS for patient safety
The starting point was the establishment of the SIMPASS (Simulation for Patient Safety) group, an interprofessional network composed of doctors, nurses, and adult training experts, coordinated by the Quality and Patient Safety Service. In particular, we wanted to hunt down errors before they could have consequences for patients, transforming real critical situations into opportunities for learning and improving our hospital system.
Right from the start, we collaborated with the Simulation Center (CeSi) of the CPS in Lugano, the reference point for healthcare simulation in the entire Canton of Ticino. Together with them, we tried to standardize the group’s methodologies for designing in situ simulations to adapt them to real clinical contexts.
None of us wanted to improvise: we had to learn how to construct realistic scenarios that were relevant to our hospital context, involving professionals directly in the departments where they work every day. We therefore began by selecting real adverse events and near misses that had occurred in the hospital as the basis for our simulation scenarios. This approach ensured that each exercise was not just abstract training, but a real stress test of the system on the specific weaknesses identified by a preliminary risk analysis. (Deutsch et al., 2024)
For us, simulation has gradually become an operational and systemic tool,
capable not only of training individual skills, but also of activating collective mechanisms of observation, reflection, and adaptation in the real contexts in which we work every day. Our annual simulation program now involves over 400 professionals and all departments, structurally integrating simulation with risk management.

From training to risk management tools
Initially, our simulations focused on clinical and training aspects. We soon realized that, in order to make a qualitative leap, we needed to incorporate structured risk analysis tools into the design cycle. We therefore began mapping the clinical processes of each scenario using methods such as SIPOC tables and flowcharts (swimlane diagrams) to clearly visualize critical phases and interactions. We then moved on to techniques such as HAZOP, BowTie, and Fault Tree Analysis. Each of these methods was tested and integrated, helping to strengthen the preventive approach of simulation.
After each simulation, we conduct a structured debriefing and collect staff observations ‘in the heat of the moment’, as this is often when hidden system gaps emerge. At the same time, we focused on organizational culture: we wanted every participant to feel safe expressing doubts and mistakes during the debriefing, without fear of blame. Over time, we have seen a tangible increase in psychological safety within the teams, with people talking openly about what went wrong and what went right, treating mistakes no longer as individual faults but as opportunities for improvement. This change in attitude is a key element of a strong safety culture supported by a high level of trust and open communication. ORBV’s experience confirms what is also emerging from the literature on high-reliability contexts (Kingston et al., 2022): to strengthen patient safety, it is essential to cultivate a culture of continuous learning based on psychological safety. For this reason, we have invested in a structured way in debriefing as a tool for reflective learning and have actively involved clinical and organizational leadership from the earliest stages.
In situ simulation has been formally integrated into the annual corporate plan for quality and patient safety,
consolidating its role not only as a training activity but also as a strategic lever for organizational development.
Structured analysis and building organizational resilience
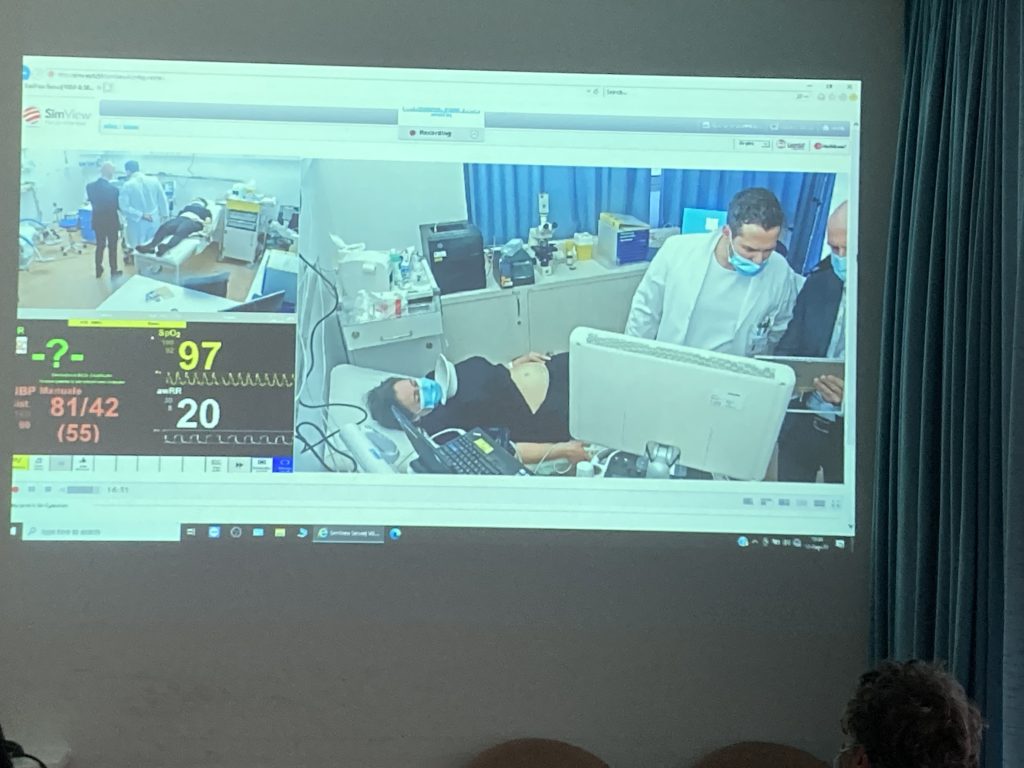
Alongside structured hot debriefings, we have introduced a second systematic ‘cold’ analysis, organized 3–4 weeks after the exercises. In these sessions, the entire team is reconvened and, through guided viewing of videos recorded during the simulated experience, the actions taken are analyzed collectively. We then enter a crucial phase of our journey: the identification of contributing factors and barriers to safety, inspired by Vincent’s factors model. Here, we do not just ask ourselves what went wrong, but we go deeper, exploring why it happened, what contextual conditions favored it, and how we can transform the experience into learning. We then analyze organizational, environmental, team, individual, and procedural aspects, looking for both the elements that hindered safety and those that promoted and supported it. This allows us to build a structured and shared assessment of the simulated event. But we don’t stop there: we translate this analysis into a “resilience map,” a tool that allows us to visualize the priorities for action within the system. Thus, step by step, we define not only what to improve, but above all where and how to act to truly strengthen our ability to deal with the unexpected.
Simulation and Safety-II: towards more resilient systems
This approach fully reflects the principles of Safety-II, as proposed by Hollnagel and colleagues (2017): the focus shifts from eliminating error to understanding the mechanisms that enable a system to adapt, compensate, and function in complex conditions. In this sense, simulation is no longer just a warning tool, but becomes a real driver of organizational learning and resilience building.
We have also noticed a virtuous side effect: operators who feel more confident in expressing themselves are also more likely to report near misses, helping to bring problems to light early and prevent serious adverse events. (Kingston et al., 2022) This synergy between training, risk management, and a positive culture has evolved simulation from simple training to a lever for continuous organizational improvement.
Final Considerations
Our approach aligns with the principles of translational simulation, where simulation is not just a training activity, but a tool designed to generate direct impact on clinical and organizational processes. (Nickson et al., 2021) Scenarios create a direct bridge between the simulation exercise and the actual clinical process, anticipating changes to safety protocols and allowing for real-time rethinking of operating procedures. We have observed how some simulations, such as those on risks during obstetric emergencies, have not only optimized behavior in emergencies but have also led to a complete overhaul of the alert code, making it more modular and immediately applicable. In this way, simulation becomes a diagnostic and transformative mechanism at the service of the system.
BIBLIOGRAPHY
Deutsch ES, Bajaj K. Simulation To Improve Patient Safety: Getting Started. Rockville, MD: Agency for Healthcare Research and Quality; July 2024. Publication No. 24-0055.
Deutsch ES, Van CM, Mossburg SE. Resilient Healthcare and the Safety-I and Safety-II Frameworks. PSNet [internet]. Rockville, MD: Agency for Healthcare Research and Quality; July 2024. Publication No. 24-0055
Hollnagel E. Safety-II in Practice: Developing the Resilience Potentials (1st ed.). Routledge. 2017
Kingston MB, et al. Annual Perspective: Psychological Safety of Healthcare Staff. PSNet [internet]. Rockville (MD): Agency for Healthcare Research and Quality, US Department of Health and Human Services. 2022.
La simulazione come strumento per la gestione del rischio in ospedale. Le strategie per ridurre al minimo i rischi di errore umano nell’ambito sanitario. Tutto Salute, Settembre 2022. https://tuttosalute.ch/wp-content/uploads/2022/10/TuttoSalute_2022_03_WEB.pdf
Nickson CP, et al. Translational simulation: from description to action. Adv Simul 6, 6 (2021).
READ ALSO