



MOSAICO, developed by Talca University in 2015, merges Computer-Supported Collaborative Learning (CSCL) and Clinical Simulation (CS) to enhance simulation-based education. It promotes advanced cognitive skills and comprehensive clinical competence through interactive collaboration and flipped learning. Participants design and assess their own scenarios, gaining a deeper understanding of clinical conditions. Successfully implemented in Chile and Spain, MOSAICO provides a 360º view of clinical competencies across various healthcare levels.
Clinical Collaborative Simulation (CCS) also known as MOSAICO was developed by Talca University (Chile) in 2015 by merging Computer-Supported Collaborative Learning (CSCL) and Clinical Simulation (CS) (Guinez-Molinos et al, 2016). It was born from a need for more effective implementation of simulation-based education and reinforced links with digitalization. Simulation could be a resource-intensive methodology. Therefore, finding way to optimize the process is a cornerstone. The complementarity between CCS and CS should allow for synergies that result in more effective teaching and learning.
MOSAICO comprises four phases:
- Phase 1: educational design by teaching staff;
- Phase 2: collaborative case design by groups of students;
- Phase 3: simulation
- Phase 4: collaborative structured debriefing
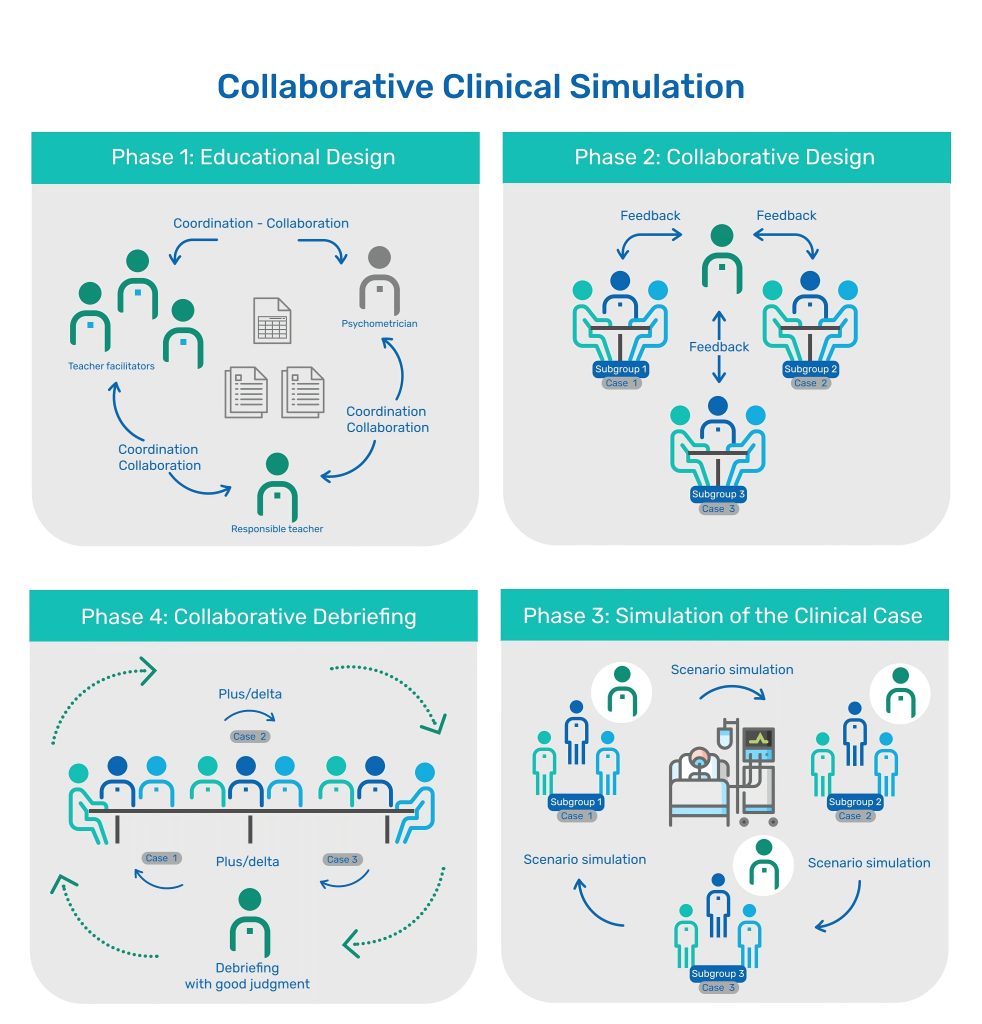
It is a method of learning and teaching designed to develop and assess clinical, procedural, attitudinal, and cognitive competencies. Furthermore, it is an innovative way where participants are going to design, assess and guide their own simulation cases.
The recommendation is to work with, at least three different diagnostics from a clinical situation (e.g.: management of patient with haematuria could be causes due to cystitis, nephritic colic, and vesical tumour). So, by being exposed to three different clinical presentations of a single clinical problem to be resolved by different groups, participants will get an almost 360º view of this clinical competence.
Phases and Implementation
During phase 1, Educational Design, a teaching committee is established to select the clinical competency to be worked on and to develop the different instruments and pedagogical guides or materials for students to review. Whenever possible, syntheses of accepted clinical guidelines and/or internationally approved performance algorithms will be used.
During phase 2, Design, it is recommended to divide participants in at least 3 subgroups of 2-5 students to facilitate interactive collaboration. Based on the materials provided before-hand and just at the beginning of this phase participants in each subgroup will design a scenario supported with guidance of a teacher. Each one of the subgroups will design a different case. They will be provided with one different clinical situation to design. The trigger could be a final diagnosis itself or a complementary test that leads to the diagnostic, if there is one (e.g.: an EKG or scan). They should think about how the clinical situation presents itself in each case and what differentiates their particular case from the others. They should develop all the symptomatology, characteristic signs and, circumstances of the patient or other roles (family members/other professionals). The group is going to distribute the roles. So, they have to think on the portrait of all circumstances in the real life to transfer them to the case.
This phase is pretty linked to “flipped learning”, since participants absorb factual content prior to class via the pedagogical guidelines developed during phase 1. Designing their own scenario cases is particularly transformative, significantly enhancing the learning process by fostering advanced cognitive skills, thereby promoting more profound and analytical thought processes in participants. Moreover, the design of case characteristics and proposed solutions will provide the students with a deeper, more integrated acquisition of clinical competence.
In the phase 3, the subgroups will take turns to be treating team, observers, and designers (they will guide the scenario) during the three scenarios. This particular way of simulation allows students to experience being in both sides of the scenario: inside as treating and designers and outside as observers alternatively. Last, phase 4 is a collaborative structured debriefing, following the different stages of any debriefing of SimZone 2, according Roussin and Weinstock (2017). Differences here lies on the fact that the three cases are equally discussed sequentially and each one of the subgroups expose their perspective from treating, designing and observers’ positions. Collaborative and team actions are discussed as cornerstones to solve patient condition. This circumstance together with realistic scenarios give a 360º view of the competence, that teacher wrap up during the closing and transferring the competence to professional life.

Outcomes and Benefits
What makes MOSAICO interesting is that participants themselves design the cases. This allows a deeper comprehension of any clinical condition, since participants must think how this clinical condition behave within that particular patient. Furthermore, the selected clinical competence it can we worked out in the different levels of health system: primary care, in-hospital care or specialized care, enriching the transfer of the competence.
MOSAICO is a highly collaborative in all different stages and genuinely participant-centred teaching methodology. It is therefore important to emphasise that the focus of the activities is on the participant, while the teacher’s role, who should have knowledge on simulation, is to guide their learning by providing advice, standards, and feedback.
So far, MOSAICO has been implemented with great success in Chile and Spain, especially with medical students. Most recently has been developed the approach for other professional such as nursing or physiotherapy, getting also great outcomes.
To have more information contact: Sergio Guinez sguinez@utalca.cl. Or go to the website: https://mosaicoweb.cl/
You can read the review of the book here.
References
Sergio Guinez-Molinos, Agustín Martínez-Molina, Carmen Gomar-Sancho, Víctor B. Arias González, Demian Szyld, Encarnación García Garrido & Patricio Maragaño Lizama. A collaborative clinical simulation model for the development of competencies by medical students. Medical Teacher. 2017;39(2):195-202. doi: 10.1080/0142159X.2016.1248913
Roussin CJ, Weinstock P. SimZones: An Organizational Innovation for Simulation Programs and Centers. Acad Med. 2017;92(8):1114-1120. doi: 10.1097/ACM.0000000000001746. PMID: 28562455.
READ ALSO











































