The Universidad Santo Tomás in Chile successfully implemented Simulation Centers across its 13 campuses to enhance healthcare education for nearly 13,000 students. This initiative, started in 2014, aimed to integrate clinical simulation into the curriculum to develop competencies using advanced technology. Read on to learn how the team that worked on the project managed to achieve this incredible milestone.
On this occasion, we want to show how we managed to implement Simulation Centers for undergraduate university students in a private institution present in 13 locations in Chile.
The challenges and aspects of this implementation were several, but here we tell you what were the main challenges we had to take into consideration for this task.
Why were Simulation Centers necessary? Because basically, it is the ideal learning method so that students in the health area, who are in their first training, can learn how to care for their patients while respecting the clinical safety of the person.
In our institution, Universidad Santo Tomás, the Clinical Simulation (CS) implementation project began in 2014, which is consistent with training based on the development of competencies, with the use of technologies that promote learning and achievement of the Graduation profile for careers in the Health area. As we mentioned before; we have thirteen headquarters or campuses from the north to the south of the country, and we had to guarantee access to simulation-based learning for nearly 13,000 students in the area.
After two years of planning and designing a clinical simulation center in terms of infrastructure, equipment and human resources, a pilot center was implemented, in the city of La Serena. Based on the simulation execution with students in this center, subsequent adjustments are made in terms of infrastructure and equipment, and they are then implemented to the rest of the centers with the improvements incorporated.
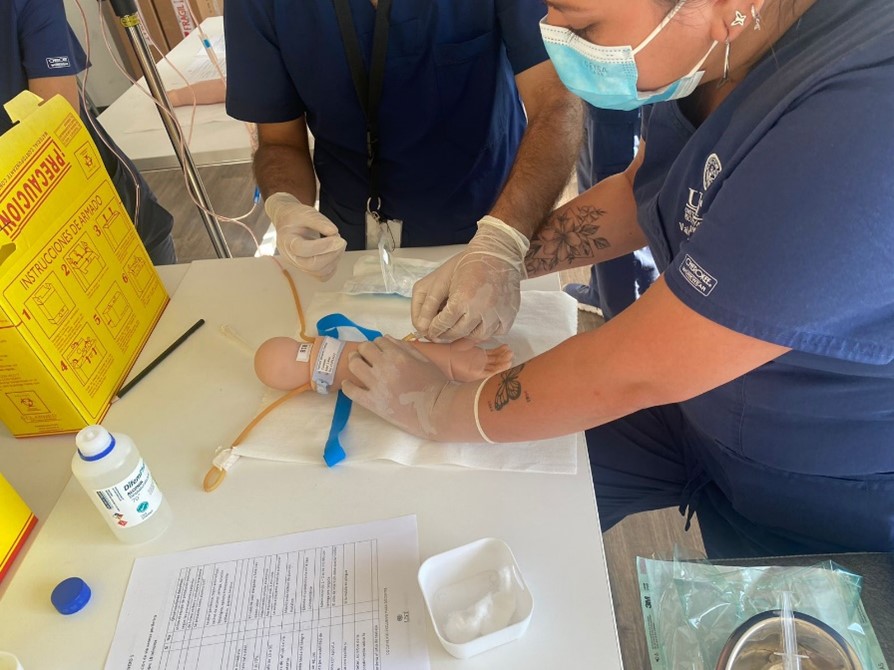
From this first experience, we not only learned about the infrastructure, but also learned the opinion of the first teachers and students regarding the methodology through a focus group with teachers who participated in the training, design and execution of the workshops, and also with the students, who carried out a satisfaction survey and an Objective Structured Clinical Examination (OSCE) to measure skill acquisition. We can highlight that, for all participants, CS is useful in the development of clinical competencies and skills, and they valued learning through error to improve safety in clinical practice. These students showed 97% satisfaction with the methodology and satisfactory academic performance in the OSCE.
At the beginning, the most challenging task was to have the material and human resources to implement the methodology uniformly in the 13 locations. To achieve this, stages of progressive implementation of both the centers and teaching were scheduled.
The institution defined five central areas for the clinical simulation unit and its implementation: curricular insertion into study plans, infrastructure design, equipment purchase, incorporation and development of human resources, and teacher training. All this in 2 stages between 2018 and 2019.
Regarding curricular insertion, the subjects that incorporate simulation are those that work on disciplinary competences in one of the training lines of each career, incorporating as criteria those that have limited times for clinical practice and have key skills for the development of professional competences.
If we talk about the infrastructure, the thirteen simulation centers are based on: rooms for workshops and scenarios, debriefing, offices, audiovisual control and warehouse, which over time have been improved in the number of rooms, depending on the number of students on campus. Therefore, some centers have more rooms than others, thus achieving 1.767 m2 built for the 13 centers in the country currently.
Another area that should be considered is the basic equipment present in all rooms to achieve the learning objectives of each degree. The large amount of equipment required designing and developing manuals, procedures, and forms for inventory control, along with equipment maintenance, purchase requests, renewal, and loans for academic activities, among others.
However, the simulation centers would not work if they did not have the human resources that manage them and continue providing methodological support and training of teachers, so in each of the Centers there is a coordinator, who is a health professional, graduate with certified training in clinical simulation. In addition, we have technical personnel, in charge and responsible for the management and care of equipment, set-up of scenarios, among other functions. To achieve uniformity in management and methodology in the 13 locations, there is a National Simulation Coordinator, who articulates the academic work with the careers for the implementation of the methodology.
Since the institution decided this, the continuous training of teachers has been relevant for teaching based on simulation and, that is why we have developed a process that begins with an induction, to then carry out courses in person and also online, in which relevant topics for facilitation, development of simulation workshops, development of evaluation guidelines, debriefing, application of teaching evaluation instruments, and finally a diploma in the area. It has been proven that becoming a facilitator implies a profound change in how the teaching experience is lived. This involves, among other things, a permanent challenge in improving the offer and coverage of simulation training.
All of this work has had a positive impact on student learning. This is demonstrated in the results obtained in a research that we developed, where a progression is evident in the acquisition of communication skills: transfer of clinical information, from lower to higher courses, related to the increase in the number of training sessions with simulation that the students have.

Therefore, it is possible to achieve high levels of performance in students, demonstrated by the ability to transfer this learning to their clinical experiences, where patient safety is ultimately impacted.
Among the projections of this unit is to install a quality accreditation system for the simulation-based education program, obtaining international certification: this team is already working towards this end.
In summary, this project has been a challenging task since its beginning, but it has been possible thanks to the team that makes it up, the trust of the authorities and the respect for the simulation that the students and teachers who participate in it have shown.
Without a doubt, we are providing tools for patient safety to future professionals and that fills us with satisfaction as a team.
READ ALSO