


Find out how ASL Roma 1 uses simulation of violence against women in the obstetrics-gynaecological emergency department to improve care for victims. This pilot experience underlines the importance of simulation-based training to prepare health professionals to deal with cases of sexual violence with competence and sensitivity. This innovative approach aims to reduce the impact of gender-based violence and to offer effective support to women in emergency situations.
In collaboration with: Anna Troiano (1), Alessandra Zannetti (1), Cristina Schirra (1), Maria Concetta Mazzeo (2), Iolanda Rinaldi (3), Maria Giovanna Colella (1), Paolo Gastaldi (1).
- Department of Women’s Health and Reproductive Physiopathology, ASL Roma 1
- UOC Training and Skills Development, ASL Roma 1
- Order of Midwives of Rome and Province
Violence against women: an endemic and pervasive phenomenon
The World Health Organisation (WHO) reports that, globally, about one third of all women have experienced physical or sexual violence by their partner or others in their lifetime. These acts of violence are mainly responsible for a whole range of health problems that women face, such as physical injuries, unwanted pregnancies, gynaecological problems and sexually transmitted infections, including HIV (WHO, 2021). In Italy, data from the National Institute of Statistics (ISTAT, 2023) inform that 31.5 per cent of women between 16 and 70 years of age have experienced some form of violence in their lifetime and, of these, 21 per cent sexual violence. An endemic and rampant phenomenon. The legislation enacted in recent years aims to strengthen a system approach by integrating non-emergency interventions, entrusted to the territory, and emergency interventions, the prerogative of the hospital and in particular of the emergency room. A complex system that provides for reporting and documentation at national level but that cannot disregard assistance to the individual woman in accordance with the national guidelines for the relief of victims of violence of 24 November 2017 (DPCM 2017). The management of the woman victim of sexual violence in an emergency is a complex and delicate path, due to the psychological, emotional, clinical and judicial implications in relation to the correct collection of biological traces and supporting photographic material, as well as the assessment of the risk of ‘revictimisation’. According to the 2017 National Guidelines, every emergency room must be able to guarantee the correct care for women victims of violence. The aforementioned Guidelines, in the annex concerning professional training, recommend an integrated strategy and also envisage the use of clinical case simulation. Simulation therefore plays an important role not only in the acquisition but also in the maintenance of the knowledge and skills of professionals. In the absence of realities that use organisational solutions such as dedicated teams or case managers, any professional on duty could find him/herself having to manage a woman victim of an episode of violence, having only theoretical knowledge and having never worked alongside a more experienced colleague. In this context, a training course for the management of the victim of sexual violence in the emergency department by means of simulation was proposed.
Effectiveness of Simulation in the Prevention and Management of Violence against Women
Simulation is a strategic resource for emergency room care of the female victim of sexual violence. In 2021, Polonko I. publishes an article in IJoHS in which he describes the use of simulation with simulated patients in the training of multi-professional healthcare teams in the management of patients who are victims of violence. In particular, the results demonstrate the effectiveness of the methodology in reducing the anxiety of staff in training and improving care. Also in the same year, Pinar G (2021) published an article demonstrating that incorporating simulation into a comprehensive domestic violence (DV) screening initiative is an effective strategy for DV prevention, recommending that simulation-based continuing education should be adopted as standard practice in health clinics.
Simulation in Violence Against Women Training: The Case of ASL Rome 1
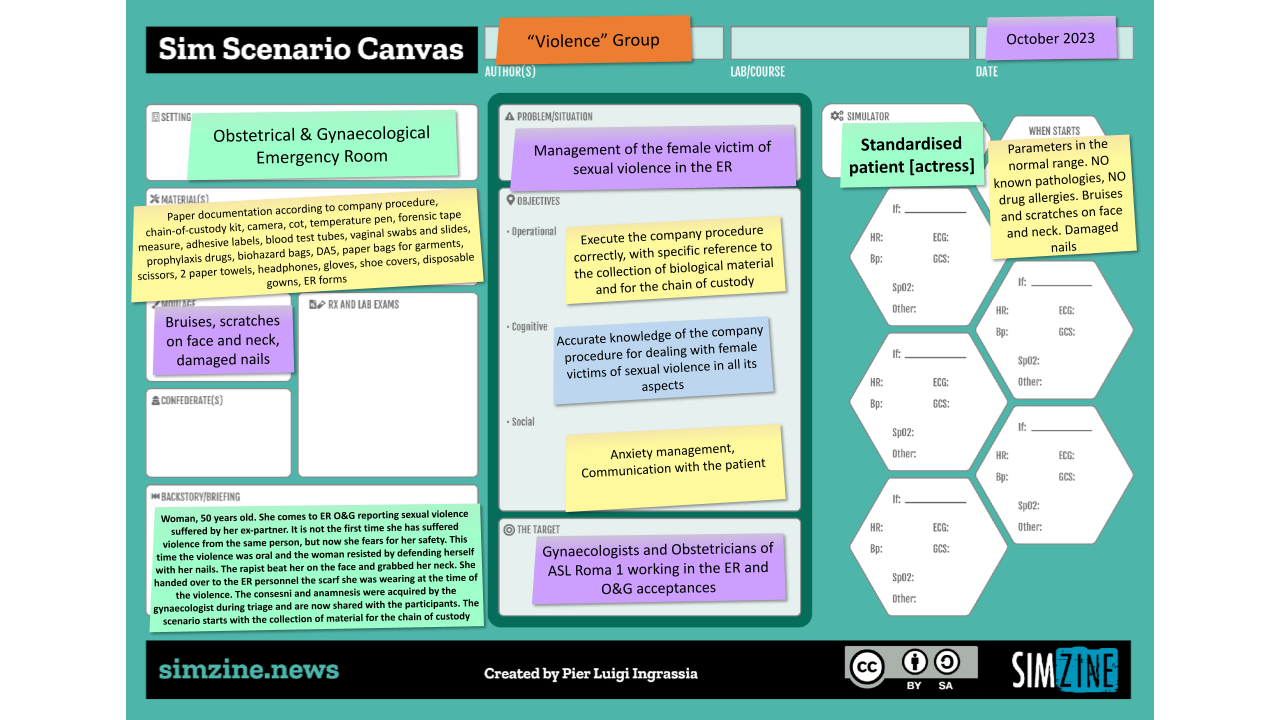
Our training initiative was preceded by a day of discussion between debriefers and facilitators to design scenarios. The Sim Scenario Canvas tool was used to design and develop the simulation scenarios, facilitating collaboration between different professionals in the application of the corporate procedure, the subject of the training day.
The training day began with a plenary discussion in which the theoretical concepts on the topic were shared and in which the phases of the reception of the woman victim of sexual violence in the obstetric-gynaecological emergency room were reviewed, identifying the strengths and weaknesses of the procedure. After familiarising themselves with the simulation environment, the learners were exposed to a clinical scenario of a team simulation with a standardised patient, i.e. a trained actress. The scenario allowed the learners to experience a realistic situation and to bring into play their technical knowledge and communication skills both with the victim and within the team. Professional role exchange was also applied in order to improve the colleagues’ awareness of their role, their priorities and how to act. In the debriefing, which followed the scenario, the trainees reflected on their actions and emotions, stimulating awareness of their knowledge and skills and aspects to be deepened and improved. In particular, the need to develop appropriate communication strategies to manage this type of patient and control emotional relapse, in relation to the relationship with the victim, emerged. Eye contact, closeness, tone of voice, acceptance, the need to devote time were aspects experienced in the simulation experience and subsequently shared and expanded upon in the critical reflection phase. The choice of role exchange given to the participants during the scenario was particularly appreciated: “playing a different professional role from the real one offered me the opportunity to experience the simulation scenario from a different perspective, seeing things from another angle and making some interesting discoveries,” reported one of the learners.
The event continued with a simulation experience in Zone 1, following the SIMZONES model. The trainees experimented with purely technical and procedural skills in a controlled environment, simulating the retrieval of clothing, biological material, and photographic images, including how to make and send the ‘chain of custody’ under the supervision of the facilitators.
The event concluded with a plenary discussion and reflection on the theme of the day’s work. Among the various proposals gathered, it emerged that the sequence of simulation activities should be modified, with the simulation in zone 1 being preceded by the clinical scenario (zone 2).
Results and Feedback
The evaluation of learning was implemented using pre- and post-training tests according to Kirkpatrick’s model (level 2). Participants and auditors provided 74% and 97.4% correct answers to the pre- and post-tests respectively, demonstrating a significant improvement in knowledge in line with expectations.
The level of learner involvement and satisfaction was very high, this was confirmed by the outcome ratings of perceived quality in relation to: relevance of the topic covered, quality of the programme and usefulness of the event. The learners expressed an interest in repeating the experience in order to gain more confidence and knowledge.
In view of the results of the first edition, a training course was developed starting in 2024 in order to guarantee systematic training of operators for the acquisition, improvement and maintenance of knowledge for the management of women victims of sexual violence in obstetrical-gynaecological emergency rooms.
Bibliography
World Health Organization (2021). Violence against women. https://www.who.int/news-room/fact-sheets/detail/violence-against-women
Istituto Nazionale di Statistica (2023). Il numero delle vittime e le forme della violenza. https://www.istat.it/it/violenza-sulle-donne/il-fenomeno/violenza-dentro-e-fuori-la-famiglia/numero-delle-vittime-e-forme-di-violenza
Decreto Del Presidente Del Consiglio Dei Ministri del 24 novembre 2017. Linee guida nazionali per le Aziende sanitarie e le Aziende ospedaliere in tema di soccorso e assistenza socio-sanitaria alle donne vittime di violenza. (18A00520) (GU Serie Generale n.24 del 30-01-2018). https://www.gazzettaufficiale.it/eli/gu/2018/01/30/24/sg/pdf
Polonko, I. ( 2021). Use of Live Patient Simulation to Train Providers on Sexual Assault Response. International Journal of Healthcare Simulation.1 (Supplement 1).
Pinar, G. (2021) The Role of Simulation-Based Education for Domestic Violence Management. Creative Education, 12, 2852-2862.
READ ALSO








































