



How to implement simulation-based training in a low-resourced setting? This is the story of a six-year journey from a rural hospital in Tanzania and how the staff managed to improve their clinical care for their non-breathing newborns through rigid, iterative quality improvement work, including a lot of simulations.
The Golden minute: a Lifesaving Race Against Time
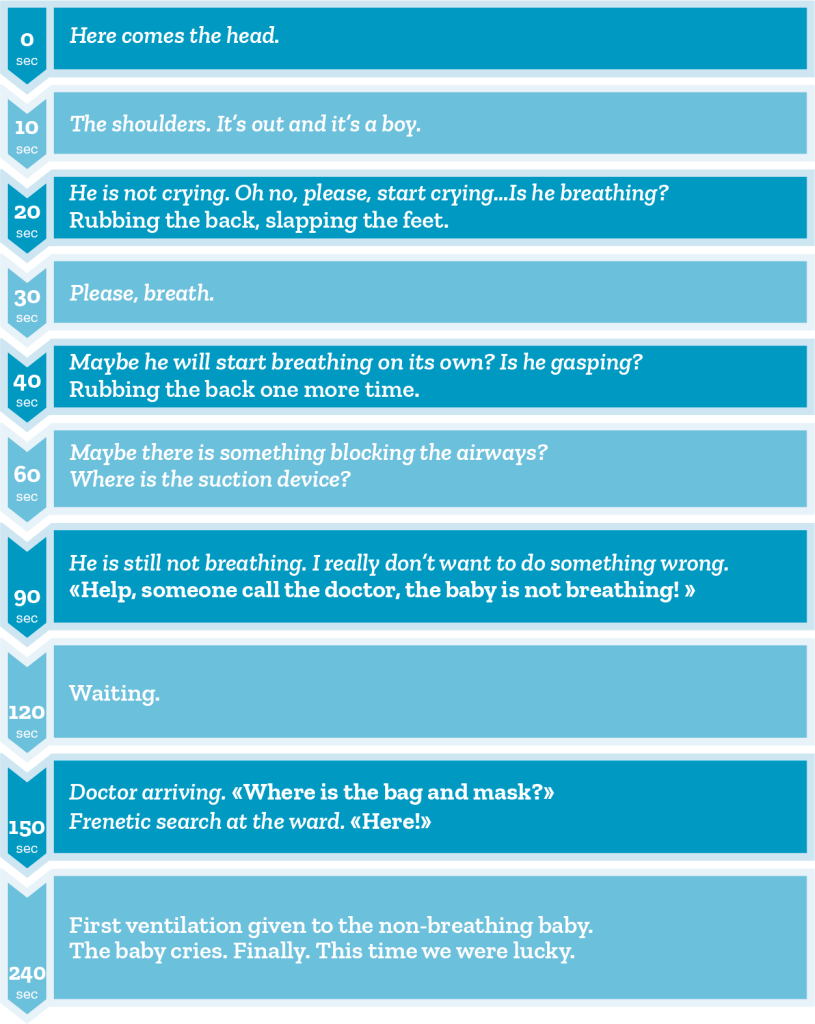
Clinical resuscitation guidelines recommend starting bag-mask ventilation of a non-breathing newborn within the first 60 seconds after birth. For each 30 seconds delay of ventilation, the risk of brain damage and death increases. Still, quickly starting ventilation is really challenging, and this goes for both high-and low resourced settings. Some studies show that less than 1% of the non-breathing newborns receive ventilations within this first golden minute of life. Recognizing a baby in need of ventilation, having the right equipment ready, mastering the technical skills of ventilating newborns and crucially, working effectively as a team are all necessary steps for reaching the goal of ventilating all non-breathing newborns within the golden minute. So how do we make sure that all these steps are implemented in our labour wards? How do we make sure that all the babies born at our ward will receive high-quality and timely ventilations if they need it? And more generally, how do we ensure implementation of clinical guidelines for all kinds of critical medical procedures in healthcare practices?
Practice Makes Perfect: The Impact of Simulation Training
If you are reading this article, you probably already know and agree on the value of simulation-based training for improving all the steps for successful newborn resuscitation listed above. Simulation can be used for training of the technical skills, and also for the non-technical skills like decision making, situation awareness and team communication. Lately, translational simulation has shown that simulation additionally can be used to find latent safety threats in the clinical setting, like lack of equipment or understaffing. In fact, simulation has already been proven to be effective in improving care for the non-breathing newborns, also in low-resourced settings. So, what are we waiting for? Just start training, or …?
I don`t know about you, but many, including myself, immediately think “That is nice, and we would all love to do that, but we just don’t have the time. We barely have time to care for our patients!”. And surely, the clinical setting is really a busy working environment, and our patients truly are the most important task. Even so, and since I am writing this to simulationists, I also know that you are among the people who already find the time to train and that you probably do advocate for its efficiency, so I hope that the story I am about to tell you will encourage you to keep doing just that.
Challenges in Low-Resource Settings
At a rural hospital in northern Tanzania, a four hours’ drive from the nearest city, Haydom Lutheran Hospital provides healthcare for a population of about 2 million people. Every year, nearly 3500 babies are born at this hospital. A dedicated staff of 20 midwives are responsible for taking care of the mother and the babies in all these cases, including the babies that do not breath at birth. That is for sure a busy work environment! To add to the picture, many of the mothers in labour arrive late at the hospital and in many cases, there are birth complications. In general, in Tanzania, 22 newborns out of 1000 liveborns die within the first month of life, about a quarter of these dying because of birth-related complications. This means that for many midwives working at this hospital, experiencing the loss of a newborn is sadly not that rare an event. And as for all healthcare workers, losing a patient is what we all fear the most. So, when Helping Babies Breathe entered the stage in 2009, providing a simulation-based training course for newborn resuscitation, Tanzania was first in line to provide the course for their midwives. The course lived up to the expectations regarding improving knowledge and skills in training for newborn resuscitation, but it failed to show translation of these training skills into improved clinical practice. Even though the midwives performed better in training after the course, they made the same mistakes when they arrived back at their labour ward caring for the real newborns. To overcome this challenge, refresher training was recommended, and Haydom implemented low-dose high-frequency skill training at their labour ward, this time showing reduction in newborn mortality! The Safer Births project investigated this intervention, among other birth-related interventions, and documented the improvements. Still, mortality rates were unacceptably high and the time from birth to start ventilation remained a challenge. Interviews with the midwives at the hospital also discovered that there was a need for a more realistic manikin and for feedback on the performance following the training. Laerdal Global Health co-designed a new manikin, the NeoNatalie Live, together with the midwives at Haydom. The new manikin was for sure more realistic, and it offered several different patient cases and importantly the manikin provided automatic feedback after training. This feedback was given in a prioritized order according to the clinical algorithm. So, when a midwife had trained, he or she would receive feedback like “Remember to tilt the head slightly backwards for open airways”. To ease the training-load, the manikin was placed in-situ, at the labour ward for the midwives to train whenever time allowed.

To assess if the training really improved the midwife’s clinical behaviour, we collected data both from the trainings but also from all the real-life resuscitations at the hospital in the following year. Trained research assistants observed every birth and recorded wide-ranging information about the mother, the labour, the newborn and crucially, the resuscitations. After a year of this self-guided training, we found that the midwives had trained two times per month and that training on the new manikin had made them better at real-life ventilations, both the technical skills, but also the time management. Actually, they had reduced the time from birth to start ventilation on real newborns from 120 seconds to 100 seconds! We also found that more resuscitations were now performed by midwives, and they were able to ventilate the newborn with less pauses, which is important for the outcome of the newborn.
But it was still not enough: Simulation-Based Training and Local Champions
Still, there were opportunities for improvement to meet the guideline requirements of non-breathing newborns ventilated within the first 60 seconds after birth. We also knew that maintaining motivation for training, and actually for most behavioral changes, is challenging in the long run. So, to meet this challenge, Haydom appointed four local champions from their labour ward, giving them the task to remind and encourage their colleagues to keep training. The local champions were junior midwives, chosen due to their positive, encouraging personalities.

These champions used every opportunity to explain the importance of high-quality ventilations and of training and they genuinely motivated their colleagues. They even arranged informal competitions, dividing the ward in two teams, competing against each other on who could train the most, and their effort really paid off. A year later, 8500 individual skill training were documented, equaling daily training for every of the 20 midwives! Also important, 75% of the midwives now participated in training every month, decreasing the performance gap between midwives at the ward. What we found when we looked at the real-life resuscitations this year, was a continued improvement in the technical skills, proving that the training was effective in this regard. But what surprised us, was the stagnation of the improvement in time from birth to start ventilation, around 100 seconds. It seemed that more individual skill training just wasn’t enough to meet the guideline requirements of the golden minute.
The Success Through Systematic Efforts
Again, the management and the staff at Haydom acted. They decided to meet the challenge with a broader approach. They launched an ambitious quality improvement campaign, the Golden Minute campaign, aiming at ventilating 70% of all non-breathing newborns within the first 60 minutes after birth. To lead the campaign, they chose their local champions. They decided to educate them as simulation facilitators, recognizing the need for adding team-simulations to their training program. The local champions conducted the EUSim Level 1 course at SAFER, Norway, learning how to write scenarios, plan, run and debrief simulation sessions. At the labour ward they initiated regular team simulations, focusing on timely, high-quality ventilation of non-breathing newborns according to clinical guidelines. An important feature of the simulations were psychological safe debriefings, focusing on reflection-based learning exploring both successes and failures. It is known that some cultures have a higher power-distance index, making it harder to speak up and a tendency to shame and blame in contrast to learning from mistakes. Introducing this new methodology was an important part of the quality improvement campaign. Additionally, the management acknowledged the importance of audit and feedback as part of quality improvement efforts, and they provided all healthcare workers with performance data from their own ward to track the progress. These data were also used to design relevant scenarios and prioritize among topics for the team training. Monthly meetings were conducted with healthcare workers and their managers to jointly discuss the data and further the challenges and successes when caring for non-breathing newborns. At the end of these meetings, action points for further improvements were agreed upon. These points for improvements addressed both clinical decision-making, structural challenges at the ward (like equipment readiness) and need for specific training sessions.

When looking at the results at the end of the campaign, a year after its initiation,
we were astonished to see that the midwives really had succeeded in changing their clinical behaviour!
69 percent of the non-breathing newborns, compared to 14 percent before the campaign, were now ventilated within the first 60 seconds of life! Time from birth to start ventilation had dramatically dropped from 101 seconds to 55 seconds. Surprisingly, we also found a reduction in the proportion of fresh stillbirths, indicating that these babies were actually severely asphyxiated, not stillborn, and therefore benefitting from rapid onset of skilled ventilations.
When asked about the most important factors to consider when implementing simulation-based training at a hospital ward, Paschal Mdoe, Hospital Director, Haydom Lutheran Hospital answered: «The local champions are the drivers of simulation activities at our hospital. They lead and inspire others to plan and use the gadgets including NeoNatalie Live. The local champions are the ones who came up with the Golden Minute Campaign that brought the staff together. Nevertheless, NeoNatalie Live has played a major role when it comes to newborn resuscitation, especially the bag-mask ventilation».
And finally, some reflections
Long story short: structured, systematic, iterative effort over time does hold the potential to change clinical behaviour and improve the care for patients. It takes time and effort, but by providing easily accessible and realistic manikins, automatic feedback and combining it with dedicated facilitators that lead the way for culture change through team-simulations, I truly think it is doable. I would also like to highlight the importance of data-guided feedback to drive system changes, including tailoring simulation sessions: it is motivating and can assist us with prioritizing our focus areas.
Finally, I want to express my deepest admiration for the staff at Haydom Lutheran Hospital. They find the time when there is none, they find the resources when they are lacking, and they show us how to work systematically with implementation of simulation and that hard work really pays off.
To wrap up this real-life story I quote Sabrina Sarangu, nurse-midwife and simulation faculty at Haydom: «The most encouraging (with the simulation activities) are the reduction of neonatal deaths in my hospital, the healthcare workers to be competent and confident, and to be able to make debriefing with non-blame culture in order to identify our gaps for continuous quality improvement».
READ ALSO







































