


Physiological models in simulation are increasingly used to support clinical reasoning, and beginning to be applied in remote monitoring and personalised healthcare. By integrating biosensors, AI, and model-driven simulators, these tools could help clinicians better understand patient responses and anticipate the effects of interventions. Richard Helyer explores current applications and future potential without overstating their capabilities.
The Rise of Real-Time Monitoring
Imagine you are at home or at work and your General Practitioner (GP) is in their practice observing your key physiological signs and variables ‘live’. You don’t know this, but using data from implanted biosensors they have been alerted to a change in your blood pressure, or levels of glucose, or heart rhythm. Using your ‘digital twin’, they explore the effects of a change in your medication or another intervention over time. Decisions are made to deal with your problem remotely, changes in drug doses are sent automatically to your online pharmacy, the settings of a device implanted in your brain are changed, or at worse a message is delivered to your smart device to call you in to your local clinic. You don’t even know you have seen your GP, and then they efficiently move on to the next patient automatically flagged to their list by Artificial Intelligence (AI).
Sounds like science fiction? All of this is based on realities that are with us now.
The technologies behind physiological models in simulation
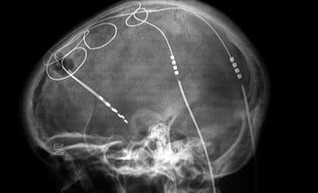
Biosensors are already widely used, or example in glucose monitoring. We can swallow an electronic ‘pill’ to explore the workings of the GI tract. Telemetry allows data from monitored variables to be uploaded to the cloud. Advances in computing and AI recognise patterns in variables, interpret the data and suggest outcomes without human intervention. Implanted devices can already change heart rate, controlled from outside the body. Electrodes providing-deep brain stimulation can control blood pressure in therapeutically resistant individuals and alleviate symptoms of degenerative disease.

Why Physiological Modelling Matters for Realistic and Predictive Simulation
But what is the role of physiological-modelling in all this? Why is it critical? And how has the world of simulation brought us closer to solving ever growing day-to-day challenges in healthcare outside of education?
All simulators are to some extent ‘digital twins’. In an Airbus A320 flight simulator, the flight deck controls and their effects on aircraft behaviour are accurately reproduced. The simulator behaves just like the real aircraft including in its response to external forces: it is a digital twin. Similarly, a simulator for the bridge of an oil tanker allows the captain and port pilot to practice berthing the ship in its dock. In engineering, digital twins are used to test how critical components will behave under stress, for example jet turbines or supporting structures for a road bridge.



Accuracy is paramount: the simulator must behave like the real thing otherwise the learning is flawed.
In the same way, in our practice of healthcare simulation we strive for realism, whether physical, haptic, behavioural, or accuracy of physiological signs and monitored signals. And here is where physiological-modelling comes in. Simulators with a physiological-model are already more-or-less a twin of our patient. Take for example the Elevate Maestro Evolve (Elevate Healthcare, Sarasota, FL, USA) model-driven human patient simulator. This allows learners to experience real-time changes in signs and signals on virtual patients, and see success or not of an intervention in real-time.

Towards Personalised Digital Twins: Top-Down and Bottom-Up Approaches
Of course, the accuracy of the responses of the twin is only as good as the data the model is based on and the accuracy of its algorithms. But already we have some ability to test the hypotheses and predictions of our learners: i.e., how will signs change with time if our patient deteriorates or when we apply a treatment? And we already have the ability to pause our twin or speed up effects and look into their future.
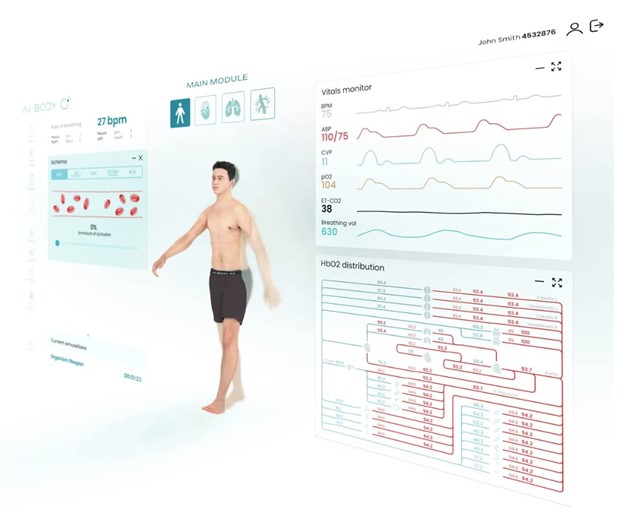
While Elevate Maestro takes a ‘top-down’ approach to physiological model allowing manipulation of key physiological parameters, for example ventricular contractility or venous capacitance, AIBody (London, UK) takes a ‘bottom-up’ approach. Here, a library of interconnected models allows manipulation of biochemical parameters at a cellular level, producing effects in tissues, organs and finally changes in monitored signals at a whole-body level.
Are digital-twins for healthcare practice a reality now? We are not quite there…yet. Current simulations are not yet rigorous enough to completely represent patients to the accuracy required to predict effects of critical interventions with safety. But we are close, already at the University of Bristol some of our teaching is based on ‘Bristol man’, a little overweight, middle-aged, somewhat hypertensive and therefore more closely a digital-twin of this author.
Conclusion
The advances made in developing physiological-models for simulation-based teaching, whether top-down or bottom-up, have set us on the road to bringing closer the reality of individual digital-twins as tools to personalise healthcare. Physiological-models are not just for simulation-based learning, but will form the foundation for patient care in the near future.
COMPETING INTERESTS
In the interests of transparency and to help readers to form their own judgements of potential bias, describe any potential competing interest (or lack thereof) for you and all contributing authors. This is simply to prevent the objectivity, integrity and value of the publication. If you are in doubt over whether you need to disclose a competing interest, consult our magazine Editor, who can guide you on the right course of action. If there are no competing interests to declare, the following statement will be added to the article “The author reports no conflicts of interest and is independent of both Elevate Healthcare & AI Body”.
READ ALSO








































