



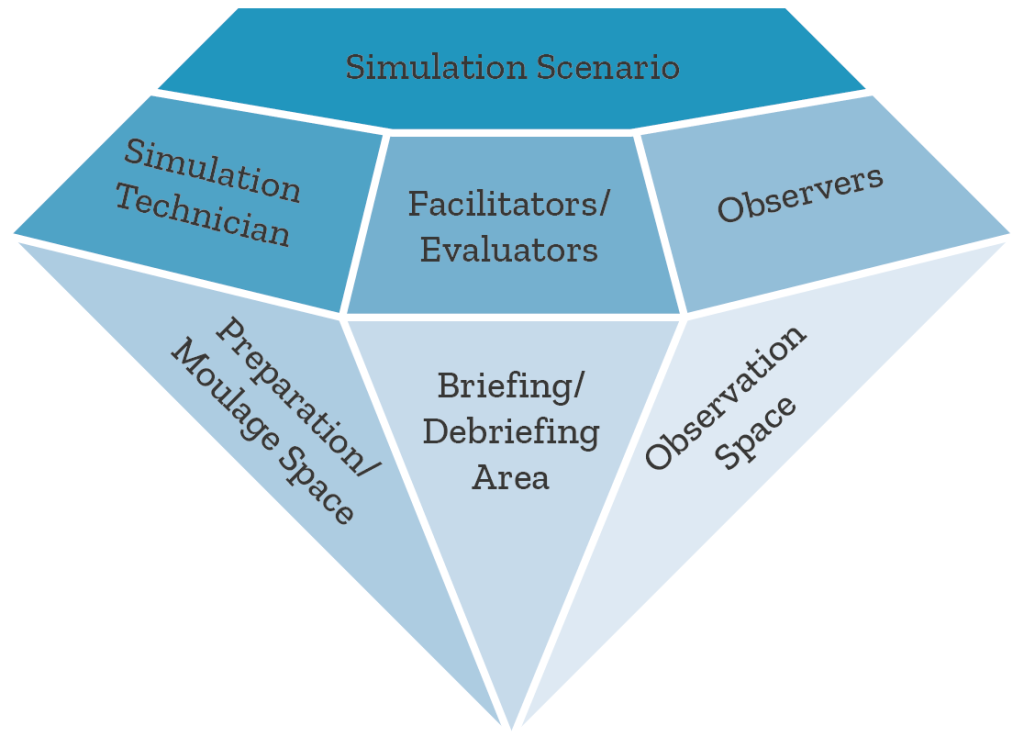
Julher Rivera Prato proposes the “Simulation Diamond,” a clinical simulation model that articulates human, technological, methodological, and spatial dimensions. This tool offers a practical guide for designing immersive, safe, and effective training scenarios, providing value to teachers, technicians, and professionals committed to quality simulation-based medical education.
Imagine you are about to begin a clinical simulation. The room is ready, the monitors are flashing, the mannequin is breathing, and an expectant team is watching you. But something doesn’t fit: there is a lack of coherence, roles overlap, and learning is diluted. What if there were a model that organized all these elements into a clear, harmonious, and effective structure? The “Simulation Diamond” was created to respond to this need, integrating the human, technical, and pedagogical aspects into a single strategic vision.
Introduction
Clinical simulation allows complex healthcare situations to be recreated in a safe environment, promoting learning, skills acquisition, and improved patient safety [1,2]. Recent studies highlight that simulation-mediated learning increases knowledge and skill retention, improves teamwork, and reduces clinical errors [3-5]. However, scenario planning still lacks visual integrative models that consider all dimensions of the process [6]. This article proposes the “Simulation Diamond” as an innovative framework that synthesizes the key elements necessary for successful clinical simulation.
Conceptual rationale
In clinical simulation, each component must contribute to a complete educational experience, integrating the human (interactions, communication, empathy), the technological (simulators, software, equipment), the methodological (instructional design, objectives, briefing/debriefing), and the physical (spaces, materiality, contextual preparation) [7,8]. The absence of any of these dimensions weakens the effectiveness of learning. The Simulation Diamond emerges as a symbolic and practical representation of this balance, where all facets are mutually reflective and work in synergy to enhance meaningful learning.
Materials and methods
A narrative literature review was conducted in PubMed, Scopus, and CINAHL, using the MeSH terms: “Clinical Simulation,” “Medical Education,” “Simulation Training,” and “Simulation Design.” International guidelines (INACSL Standards of Best Practice, SSH Accreditation Standards) were analyzed, and international simulation experts were interviewed.
Based on these inputs, the Diamond model was designed.
Results
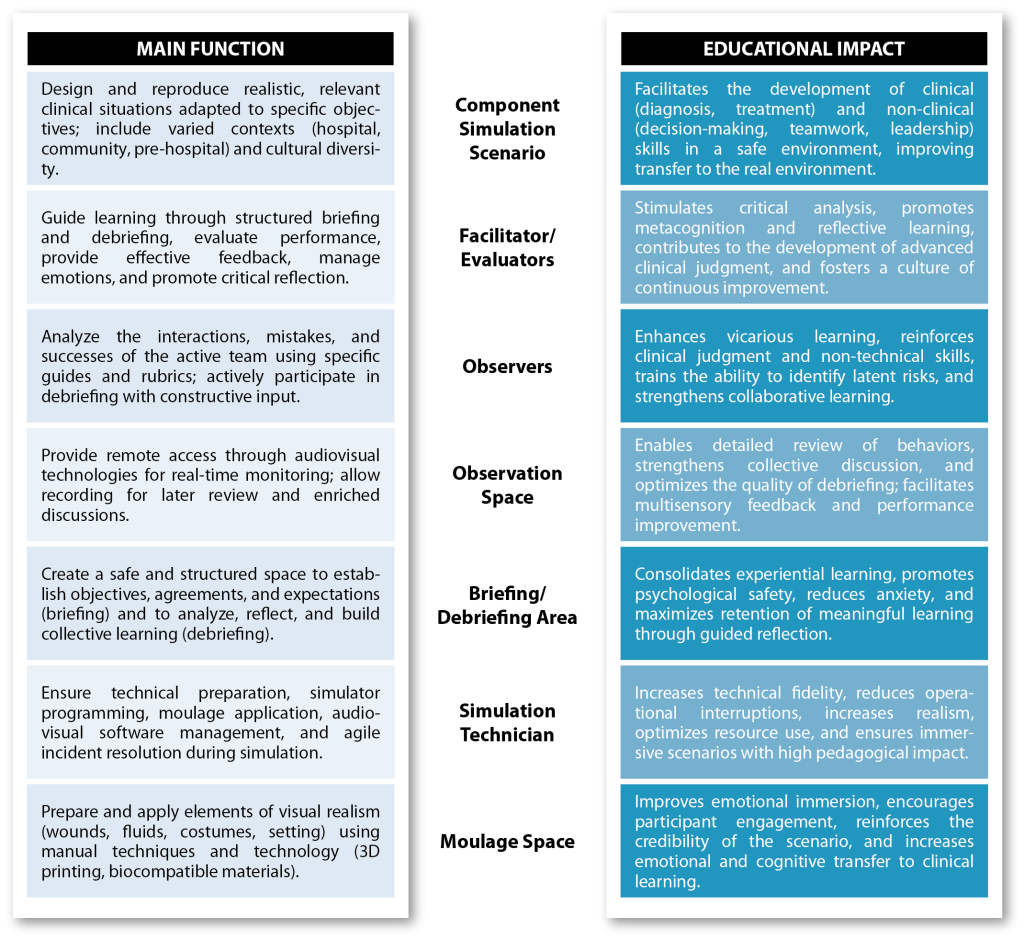
Expanded components The Diamond model integrates seven essential components, each expanded in detail:
- Simulation Scenario: This is the operational heart of the model. It requires the precise construction of clinical cases, contextual fidelity (high or low depending on objectives), and close alignment with learning outcomes. Here, decision-making, technical skills, communication, and teamwork are practiced under controlled conditions [1,2].
- Facilitators/Evaluators: These are educational leaders who fulfill multiple roles: instructional designers, performance observers, and drivers of critical analysis during debriefing. They must be trained in feedback strategies, emotional management, and methodologies such as PEARLS or debriefing with good judgment [3,4].
- Observers: They are not mere spectators; their role requires training to recognize team dynamics, detect latent errors, and extract lessons applicable to their future practice. They learn to use observation guides and actively participate in the subsequent analysis.
- Observation Space: This includes audiovisual technology (cameras, microphones, monitors) and allows observers, teachers, and technicians to follow every detail in real time. This space facilitates the generation of audiovisual evidence that will be used in subsequent reflection, strengthening learning [6].
- Briefing/Debriefing Area: This is not just a physical space, but an emotionally safe environment. Here, rules, confidentiality agreements, and scenario objectives are established, and then in-depth analysis is carried out, where meanings are constructed and the experience is transformed into learning [7].
- Simulation Technician: This is the invisible pillar of the model. This professional ensures the correct functioning of the simulators, programs physiological responses, manages software and audiovisual equipment, and creates realistic effects through moulage. Their role is indispensable for achieving high fidelity and operational fluidity [8].
- Preparation/Moulage Space: This is where the scene comes to life: wounds, bleeding, burns, costumes, and environmental details that immerse participants in a realistic clinical setting. Well-executed moulage increases emotional immersion and strengthens the connection between learning and real practice [9].
Comparative Table
Discussion
The Simulation Diamond highlights often underestimated components, such as the role of the technician and physical spaces, showing their relevance to successful learning. Failure to integrate these elements can limit the educational impact [6-9]. This model provides an adaptable practical framework as a planning, training, and auditing tool.
Limitations
The model requires advanced material resources, trained personnel, and adequate technological infrastructure, which may restrict its applicability in low-resource settings. It also demands efficient interprofessional coordination and institutional commitment, and needs empirical validation through multicenter studies [10].
Conclusion
The “Simulation Diamond” is not just a visual model: it is a strategic tool that allows for the integration of all the essential dimensions of simulation-based learning. Its value lies in highlighting frequently underestimated elements and offering a practical framework for the planning, evaluation, and continuous improvement of training experiences. At a time when simulation is becoming increasingly prominent in healthcare education, this model can become a benchmark for those seeking educational excellence with a real impact on patient safety.
REFERENCES
- Cheng, A. et al. (2016). El enfoque PEARLS (Promoción de la Excelencia y el Aprendizaje Reflexivo en Simulación) para la sesión informativa sobre atención médica: Guía de desarrollo docente . Simulación Clínica en Enfermería , 12 (10), 419-428. https://doi.org/10.1016/j.ecns.2016.05.002
- G. Díaz MC, Walsh BM. Educación basada en telesimulación durante la COVID-19. Clin Teach. 2020 Oct 12. doi:10.1111/tct.13273.
- O’Regan, S. et al. Roles del observador que optimizan el aprendizaje en la educación mediante simulación sanitaria: una revisión sistemática. Adv Simul 1 , 4 (2016). https://doi.org/10.1186/s41077-015-0004-8
- Kolbe M et al.. Briefing and debriefing during simulation-based training and beyond: Content, structure, attitude and setting. Best Pract Res Clin Anaesthesiol. 2015;29(1):87-96. DOI: 10.1016/j.bpa.2015.01.002
- Dinh A et al. Augmented Reality in Real-time Telemedicine and Telementoring: Scoping Review. JMIR Mhealth Uhealth 2023;11:e45464. URL: https://mhealth.jmir.org/2023/1/e45464 DOI: 10.2196/45464
- INACSL Standards Committee. Healthcare Simulation Standards of Best Practice. Clin Simul Nurs. 2021;58:S1-S64. DOI: 10.1016/j.ecns.2021.10.005
- Rudolph JW et al. There’s no such thing as “nonjudgmental” debriefing: A theory and method for debriefing with good judgment. Simul Healthc. 2006;1(1):49-55. DOI: 10.1097/01266021-200600110-00006
- Tellefson F et al. The role and impact of the simulation technician in health science higher education: A scoping review. Clin Simul Nurs. 2025;100:101695. doi: 10.1016/j.ecns.2025.101695.
- DCosta, S. et al. El impacto del modelado en la experiencia de los estudiantes en la educación y formación basadas en simulación: revisión sistemática. BMC Med Educ 24 , 6 (2024). https://doi.org/10.1186/s12909-023-04976-w
- Lateef F. Simulation-based learning: Just like the real thing. J Emerg Trauma Shock. 2010;3(4):348-52. DOI: 10.4103/0974-2700.70743
READ ALSO









































