



The medical field faces significant gender and racial inequities, particularly in leadership roles, despite progress in reducing disparities. Promoting diversity, equity, and inclusion (DEI) in medical education can enhance patient care by improving cultural competency and reducing health disparities. Dive into the article to gain further insights.
Introduction
The medical field, despite its advancements, continues to grapple with issues of gender and racial/ethnic inequities. While there has been progress in reducing gender disparities over recent decades, significant gaps persist, particularly in leadership roles. This essay takes a closer look at the importance of diversity, equity, and inclusion (DEI) in medical education, highlighting the challenges faced by women and minorities and proposing strategies to foster a more inclusive environment.
Gender Inequities in the Medical Profession
Persistent Gender Disparities
Despite strides toward gender equality, the United Nations Women’s report indicates that women are still restricted from certain industries in almost 50% of countries, based on a sample from 93 nations. (1) This statistic underscores the pervasive nature of gender bias that transcends borders and industries, including the medical field. The medical profession is not exempt from these disparities. Although there is equal representation of genders in medical schools, women remain underrepresented in significant academic and leadership positions, with minority women facing even greater challenges. This underrepresentation has far-reaching implications, affecting not only career advancement but also the overall dynamics and decision-making processes within the medical field. (2)
Role Models and Leadership Aspirations
Role models play a crucial role in shaping leadership aspirations. The adage “you can’t be what you can’t see” underscores the importance of visible role models for women and minorities. Unfortunately, the medical field still struggles with providing diverse role models. For example, text-to-image AI tools consistently portray heads of anesthesia departments as exclusively male, underscoring the widespread gender bias. (3) This is unsurprising, given that the initial datasets used to train large language models often included images of women from the internet, which frequently originate from pornographic content.
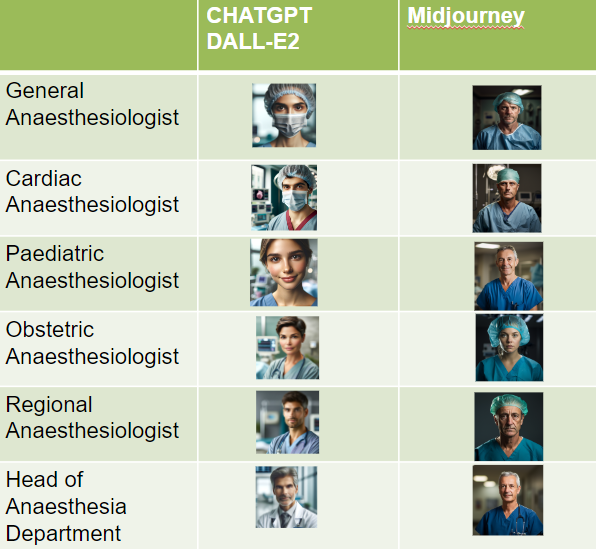
Image reproduced with permission (3)
This lack of diverse representation can dissuade women and minorities from pursuing leadership roles, perpetuating a cycle of underrepresentation and inequality.
The visibility of role models is particularly critical in the formative years of one’s career. When aspiring medical professionals see individuals who look like them and share similar backgrounds in positions of power, it instills a sense of possibility and ambition. Conversely, the absence of such role models can lead to feelings of isolation and the belief that certain achievements are unattainable. This highlights the need for intentional efforts to showcase diverse leaders within the medical field.
Medical Culture and Leadership Norms
Competitive Individualism and Masculine Norms
The medical culture often celebrates competitive individualism and masculine norms of leadership. Leaders are expected to exhibit “agentic” qualities such as assertiveness, confidence, and independence, which are traditionally associated with masculinity. Ideal code leadership, for example, is often embodied by highly agentic, stereotypically male behavior (loud, assertive and confident). This preference for agentic qualities can create a hostile environment for women and minorities who may not conform to these expectations. In contrast, “communal” qualities like cooperation, team-focus, and empathy, typically perceived as feminine, are less valued in professional success. (2) This dichotomy between agentic and communal qualities perpetuates a biased view of leadership that marginalizes those who do not fit the traditional mold. The emphasis on agentic qualities can also lead to a narrow definition of success, ignoring the valuable contributions of those who excel in communal roles.
The Double Bind for Women Leaders
Research indicates that women leaders face a double bind: they are either seen as lacking competence if they do not display agentic qualities or are penalized for displaying dominance. This dilemma forces women to juggle between communal qualities, which are preferred in women, and agentic qualities deemed necessary for leadership success. This conflict hinders women’s career aspirations and recognition.
The double bind phenomenon is not limited to the medical field; it is prevalent across various industries. Women who exhibit agentic behaviors may be labeled as aggressive/unlikable and bossy, while those who display communal traits are often perceived as lacking the necessary drive for leadership. This paradoxical expectation places an undue burden on women, requiring them to navigate a minefield of conflicting expectations. Indeed, women leaders are expected to be competent and caring, while men are expected to be competent only. (4) As a result, many talented women may opt out of pursuing leadership roles altogether, further entrenching gender disparities.
The Leaky Pipeline Phenomenon
The metaphor of the leaky pipeline illustrates how women, despite having the same professional aspirations as men, make career choices that result in disparities. Women tend to gravitate towards fields like education or community improvement, which align more with communal values but are perceived as less prestigious and lower-paying. This trend is influenced by the “Pollution Theory,” which suggests that fields aligning with traditionally feminine values lose prestige and salary over time. Without awareness and action, women’s contributions will continue to be undervalued.
The leaky pipeline phenomenon is a multifaceted issue that requires a comprehensive approach to address. It involves not only encouraging women to pursue and persist in competitive fields but also challenging societal perceptions that devalue communal roles. Efforts to rectify this issue must begin early in the educational journey, fostering a culture that values diverse career paths equally. Additionally, creating policies that support work-life balance and equitable pay can help retain talented women in the workforce.
Addressing Gender Bias and Promoting Alternative Leadership Styles
Raising Awareness
Raising awareness about unintentional social constructs and stereotypes is essential to identifying and preventing gender biases. Understanding that leadership can encompass alternative styles, compatible with the emerging idea of healthcare leadership as team play, is crucial for fostering a more inclusive environment. Educational programs and workshops that focus on implicit bias, gender dynamics, and inclusive leadership can help shift perceptions and behaviors. Institutions must also be proactive in implementing policies that promote gender equity, such as flexible work arrangements, parental leave, and transparent promotion criteria. By creating a supportive environment that values diverse leadership styles, the medical field can benefit from the full range of talents and perspectives.
The Impact of Imposter Syndrome
Imposter Syndrome in Medicine
Imposter Syndrome, defined as the inability to internalize success and the tendency to attribute it to external causes, affects many in the medical profession, particularly female physicians and those in training.
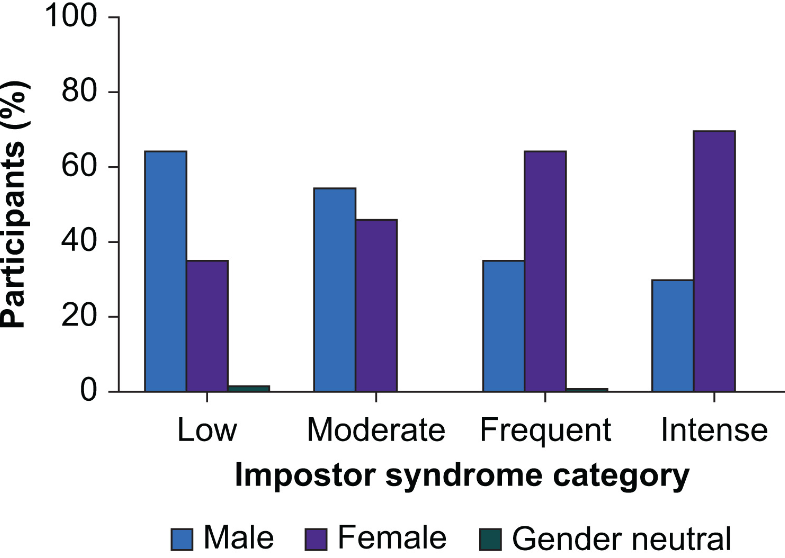
Image reproduced with permission (5)
This syndrome is linked to low self-esteem, fear of speaking up, and even burnout, impacting self-evaluation, feedback sessions, and the (lack of) development of one’s leadership style.
The high-stakes environment of the medical field can exacerbate feelings of inadequacy and self-doubt. Physicians are often held to exceptionally high standards, and the pressure to perform flawlessly can be overwhelming. For women and minorities, these pressures are compounded by the additional challenge of navigating a biased system. Addressing Imposter Syndrome requires a multifaceted approach, including fostering a supportive work environment, providing access to mental health resources, and encouraging open discussions about failure and resilience.
Combating Imposter Syndrome Through Mentorship
Mentorship is a key strategy to combat Imposter Syndrome. Unfortunately, ethnic disparities can affect the ability to find mentorship, as individuals from underrepresented ethnic groups may face stereotypes or prejudices that hinder their access to mentorship networks crucial for career advancement. Mentorship provides a vital support system, offering guidance, encouragement, and opportunities for professional growth. Effective mentorship relationships can help individuals build confidence, navigate challenges, and develop their unique leadership style. Institutions should prioritize creating mentorship programs that are inclusive and accessible to all, recognizing the unique needs of women and minority physicians. By pairing mentees with mentors who understand and can relate to their experiences, these programs can help mitigate the effects of Imposter Syndrome and foster a sense of belonging and empowerment.
Ethnic Disparities in Medical Education
Challenges in Accessing Mentorship
Research highlights the challenges minority physicians face in accessing mentorship networks. These biases result in unequal access to mentorship and professional development opportunities. Moreover, different communication styles, expectations, and approaches to networking among ethnic groups can create barriers to effective mentor-mentee relationships. Addressing these challenges requires intentional efforts to create inclusive mentorship opportunities. Institutions should actively recruit and retain a diverse faculty to serve as mentors, ensuring that all trainees have access to role models who can provide relevant and relatable guidance. Additionally, providing cultural competency training for both mentors and mentees can help bridge communication gaps and foster mutual understanding and respect.
Proactive Efforts to Bridge Cultural Gaps
Addressing ethnic disparities requires proactive efforts from both individuals and institutions. Mentors and mentees must work to bridge cultural gaps, foster understanding, and build supportive relationships based on mutual respect and trust. Initiatives like mentorship programs tailored to the needs of minority trainees, diversity training for mentors, and proactive recruitment of underrepresented faculty members can help bridge the gap in mentorship access.
Creating a more inclusive mentorship environment involves not only addressing existing biases but also proactively supporting the professional development of minority physicians. This can include providing access to networking opportunities, leadership training, and resources that specifically address the unique challenges faced by underrepresented groups. By investing in the growth and success of minority physicians, the medical field can benefit from a more diverse and dynamic leadership.
Enhancing Patient Care Through Diversity
Representation and Patient Trust
Patients from diverse ethnic backgrounds often feel more seen and understood by physicians who share similar cultural or ethnic experiences. This shared understanding can build trust and improve patient-physician communication, leading to better health outcomes. When patients see themselves reflected in their healthcare providers, it can alleviate feelings of marginalization and enhance their overall healthcare experience. Representation in the healthcare workforce can play a crucial role in patient engagement and adherence to treatment plans.
Cultural Competency and Health Equity
Cultural competency in healthcare refers to the ability of providers to effectively deliver healthcare services that meet the social, cultural, and linguistic needs of patients. A diverse physician workforce is better equipped to address the unique health concerns of various populations, including understanding cultural nuances that may affect health behaviors and treatment preferences. Recent research has raised concerns about the discrepancies between pulse oximetry (SpO2) readings and actual arterial oxygen saturation (SaO2) in individuals with darker skin tones, which can result in undiagnosed hypoxemia in these patients. (6)
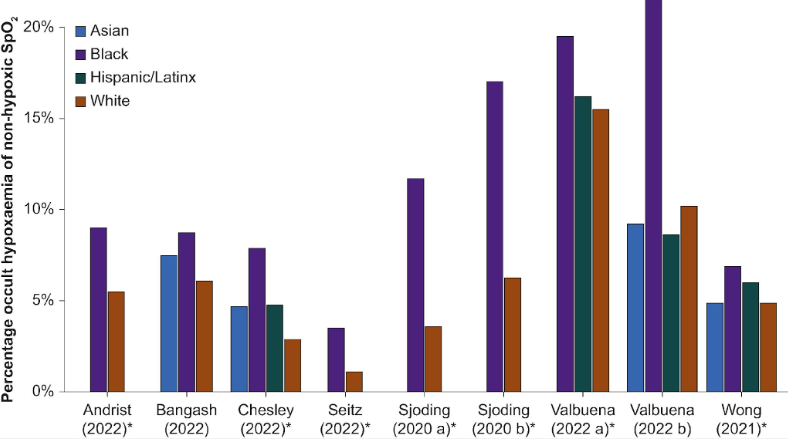
(Figure reproduced with permission (6))
A physician who is culturally competent and possibly shares a similar background can provide more tailored advice and interventions, recognizing the social determinants of health that influence these conditions.
Reducing Health Disparities
Health disparities are differences in health outcomes and access to healthcare services among different population groups. These disparities are often influenced by social, economic, and environmental factors. A diverse healthcare workforce can help reduce these disparities by providing more equitable care. Physicians from minority backgrounds are more likely to work in underserved areas and care for disadvantaged populations. This can help bridge the gap in healthcare access and quality for marginalized communities. By addressing the specific needs of these populations, diverse physicians can contribute to reducing health disparities and promoting health equity.
Conclusion
In conclusion, the importance of diversity, equity, and inclusion (DEI) in medical education cannot be overstated. The challenges faced by women and minorities in the medical field are complex and multifaceted, requiring a comprehensive approach to address. By fostering an inclusive environment that values diverse leadership styles, providing robust mentorship opportunities, and actively addressing implicit biases, the medical profession can create a more equitable and dynamic field. This will not only benefit individual physicians but also enhance the overall quality of care provided to patients, reflecting the diverse needs and perspectives of the communities they serve.
References
1- https://www.unwomen.org/sites/default/files/2024-01/e.cn_.6.2024.3_-_advance_unedited_version.pdf
2. Gender equity in anesthesia: is it time to rock the boat? Gisselbaek M, Barreto Chang OL, Saxena S. BMC Anesthesiology 2023 (PMID: 36882715)
3. Gisselbaek M, Koselerli E, Suppan M, Minsart L, Meco BC, Albert A et al. Gender Bias in Artificial Intelligence (AI)-Generated Anaesthesiologist Images. Br J Anaesth 2024 (PMID: 38942642)
4. Johnson WB, Smith DG, Christensen H. Where Women’s Leadership Development Programs Fall Short. HBR 2023 https://hbr.org/2023/03/where-womens-leadership-development-programs-fall-short
5. Impostor syndrome in anaesthesiology primarily affects female and junior physicians. Gisselbaek M, Hontoir S, Pesonen AE, Seidel L, Geniets B, Steen E, Barreto Chang OL, Saxena S. Br J Anaesth 2023 (PMID: 37884406)
6. Martin D, Johns C, Sorrell L, Healy E, Phull M, Olusanya S et al. Effect of skin tone on the accuracy of the estimation of arterial oxygen saturation by pulse oximetry: a systematic review. Br J Anaesth 2024; 132: 945-956. (PMID: 38368234)
READ ALSO









































